Fraudtism
Unmasking the Incentive-Driven Surge in Autism Diagnoses

TL;DR
Autism diagnoses have surged dramatically, but the increase largely reflects diagnostic reclassification (autism rising on SSI records as intellectual disability falls), broader criteria, and institutional incentives—not a sudden biological epidemic. California stands out: prevalence reaches up to roughly 1 in 19 in some areas (well above the national average), its developmental services caseload has ballooned, and special education enrollment has climbed even as overall student numbers dropped, creating persistent staffing shortages. I coined “fraudtism” to describe how financial rewards—disability payments, special education funding, and state programs—can encourage diagnostic inflation, especially in immigrant-dense, low-income districts. Overt fraud appears in Minnesota Medicaid kickback scandals, while subtler pressures ‘medicalize’ poverty and expand bureaucracies nationwide. A rational fix requires clearer classification (profound vs. mild), cross-cultural audits, and incentives realigned toward targeted recovery rather than endless caseload growth.
Diagnostic Substitution: From Intellectual Disability to Autism
As a primary care physician old enough to remember when “autism” was not even in use in medicine (let alone a sprawling diagnostic empire), I came to this topic a year ago, driven by pure curiosity. My public-health investigative journalism started before COVID when I began Overturning Zika: The Pandemic That Never Was.
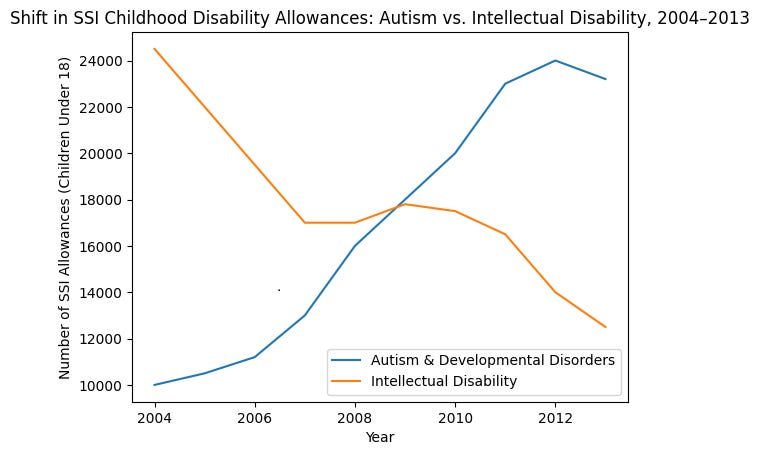
My essay, Unraveling Autism’s Surge: Genetics, Environment, and the Expanding Diagnostic Net, examined the data behind the dramatic rise in autism diagnoses and highlighted institutional incentives. One clear pattern is diagnostic substitution: federal SSI childhood disability allowances for autism and related developmental disorders rose sharply between 2004 and 2013, while allowances for intellectual disability fell by almost the same magnitude. The shift suggests reclassification rather than a sudden biological epidemic.
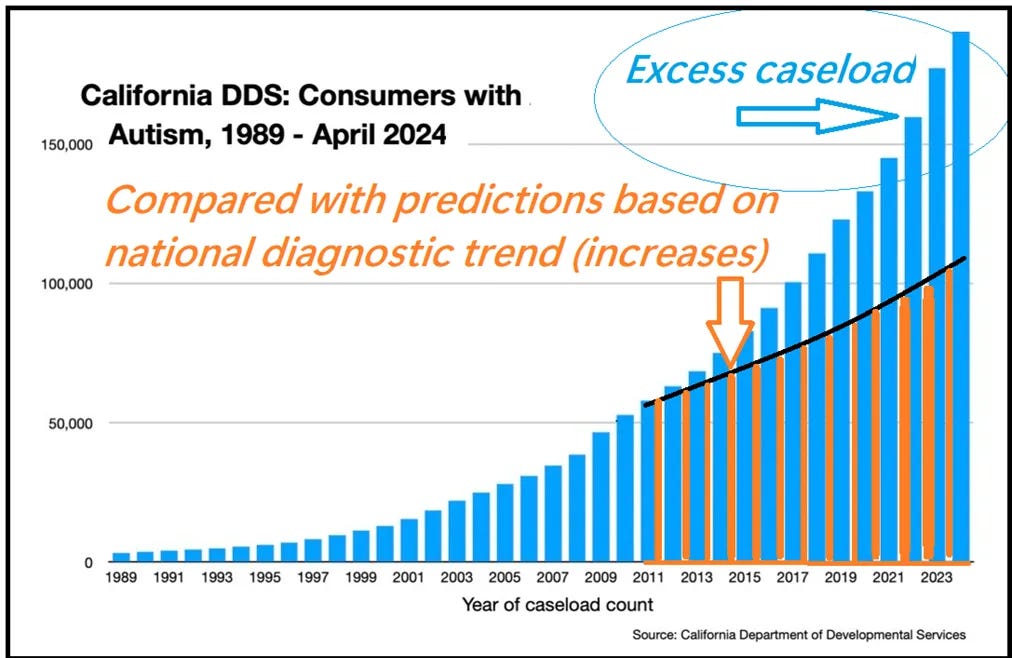
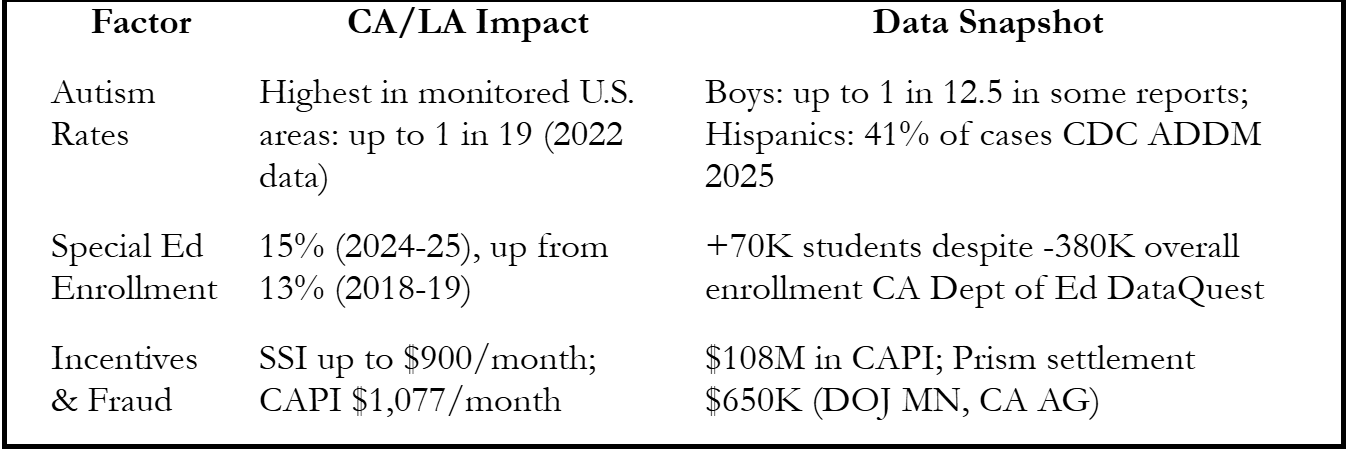
California exemplifies the broader dynamics. The state reports some of the highest autism prevalence in the country—up to roughly 1 in 19 children in certain monitored areas (2025 CDC ADDM report, 2022 data) compared with the national average of 1 in 31. Its Department of Developmental Services autism caseload reached 196,000 in 2024 (up 156% in a decade), now comprising 51% of developmental disabilities (up from 31%). Special education enrollment climbed to 15% in 2024–25 (from 13% in 2018–19) despite a drop of 380,000 in overall K-12 students, creating “crisis-level” staffing shortages.
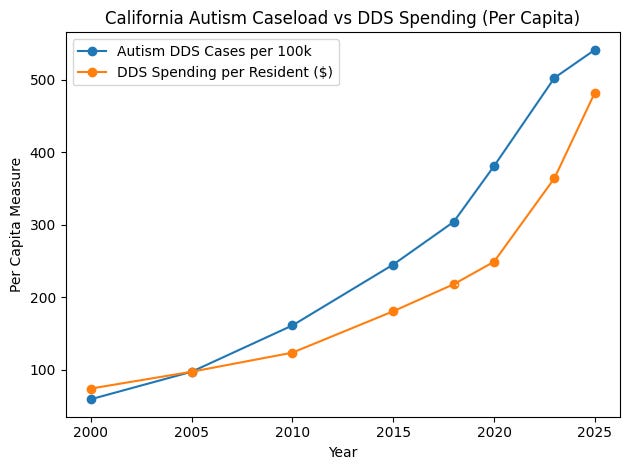
When normalized for population, California’s Department of Developmental Services’ autism-related -caseload and -spending (per resident) has climbed tenfold(!).
The Birth of “Fraudtism”: Incentives Over Biology
I recently coined the term “fraudtism” to describe the possibility that part of the surge reflects financially incentivized diagnostic inflation rather than purely biological change. The word does not dismiss genuine autism; it points to the machinery around the diagnosis. I arrived at the portmanteau independently, though fraudtism has appeared in a handful of isolated X posts and in Age of Autism coverage

of Minnesota’s Somali “lear(n)ing center” scandals.

There, autism Medicaid claims exploded from $3 million in 2018 to $399 million in 2023, fueled by kickbacks (roughly $1,000 per month per child) for fake enrollments.
My implied use of the term is broader: that financial incentives attached to certain diagnoses may encourage diagnostic expansion even where no overt criminal conspiracy exists. In immigrant-dense urban districts the pressures are easy to see. Language barriers, poverty, classroom disruption, and cultural unfamiliarity already strain schools. An autism classification brings additional teachers, specialized services, and in some cases eligibility for federal disability benefits such as Supplemental Security Income of ~$1000/month (even if parents are illegal, as long as they are born here).
School systems themselves can classify a child under the autism category for special education purposes through internal evaluation teams. When staffing, services, and potential benefits align, diagnostic expansion is inevitable even without Somali-style organized fraud. The fallout includes diversion of resources from children with severe developmental disability; false reinforcement of perceptions of a rapidly expanding epidemic; and panicked blame-games.
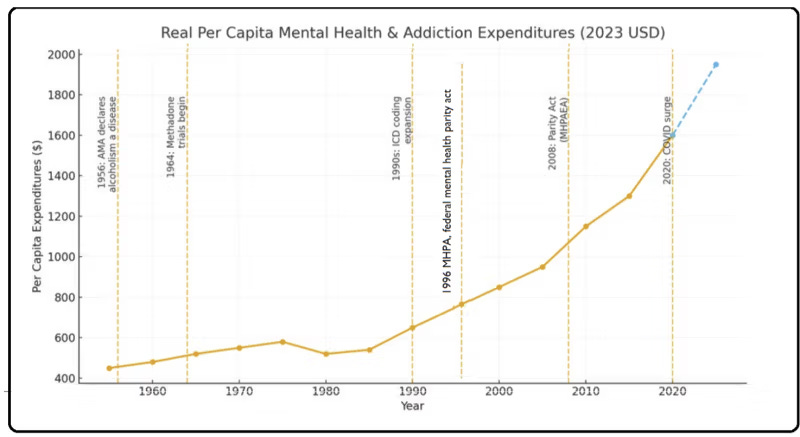
Mental Health Parity: Opening the Door to Elastic Diagnoses
Mental health parity laws, as I discussed in The Hidden Cost of Mental Health Parity, did more than equalize coverage between mental and physical illness. Historically, insurance reimbursed conditions that could be directly verified through pathology, imaging, laboratory findings, or clear physiological impairment. Parity laws opened the door to covering conditions defined largely through behavioral criteria, clinical interpretation, and subjective reporting. What began as a humane effort to expand treatment also created a system in which diagnoses that lack clear biological markers became reimbursable, billable, and in many cases lifelong.
As Humpty Dumpty declares in Through the Looking-Glass, “When I use a word, it means just what I choose it to mean, neither more nor less.” When diagnostic language becomes elastic and financial incentives attach to particular labels, the meaning of the label itself inevitably begins to stretch.
California’s Crisis: Skyrocketing Rates and Special Ed Bloat
The administrative and labor consequences are visible throughout the state. Teachers unions increasingly describe special education caseloads as unsustainable and have demanded additional hiring and resources. During San Diego’s 2026 labor dispute, union leaders cited rising special education obligations as a major driver of staffing demands. When classification rates climb faster than enrollment, the result is pressure to expand staffing, programs, and budgets in order to maintain compliance with federal and state mandates.

A parallel dynamic appears in disability payments. California operates programs that extend benefits beyond the federal system. One example is the Cash Assistance Program for Immigrants, or CAPI, which provides disability related payments to certain non citizens who are not eligible for federal Supplemental Security Income. Los Angeles County alone receives roughly $100 million per year in state funding for this program. In May 2025, Homeland Security Investigations issued a Title 8 subpoena to Los Angeles County seeking records related to CAPI as part of an inquiry into disability benefit eligibility. Investigators are examining whether individuals who were ineligible for federal disability payments may nevertheless have received them.
Fraud investigations occasionally surface as well. In one recent example the Prism Autism Foundation reached a settlement of roughly $650,000 over allegations of fraudulent autism related billing. Such cases are not necessarily representative of the system as a whole, but they illustrate the financial incentives that can arise when diagnostic classifications unlock substantial public funding.
Several of California’s highest reported autism rates occur in heavily immigrant regions. For example, the DDS report notes: “Imperial county has the highest proportion of individuals with a diagnosis of ASD (1.21% of the estimated county population), while Sierra and San Francisco counties have the lowest proportions (0.13% of each estimated county population). The statewide average prevalence is 0.46%.”
Autism diagnoses among Hispanic children historically had been lower (because families feared interaction with public agencies?). As screening expanded and policy barriers eased, diagnoses among Hispanic children rose rapidly. Some of this increase may reflect recognition of previously missed cases; yet, these trends illustrate how a diagnostic category can grow within a larger ecosystem of funding formulas, legal mandates, and service programs. Rising diagnoses, expanding budgets, and growing administrative structures reinforce one another.
A Path Forward: Target Real Cases, Curb the Abuse
The problem is not autism itself but the system that has grown around the diagnosis. When incentives expand faster than oversight, classification can drift. Mild developmental differences become medicalized, resources are spread thinly across expanding caseloads, and the most severely affected individuals risk receiving less attention than they require. In this environment, poverty and social disadvantage can be recast as clinical pathology while public spending rises without corresponding improvements in health.
A more rational approach would begin by restoring clarity to the diagnostic landscape. One step would be to distinguish more explicitly between profound autism and milder developmental conditions that may require different levels of intervention. Cross cultural comparisons could also help determine how much of the apparent surge reflects biological change versus differences in screening, service availability, and administrative practice. Most importantly, policy should shift from maintaining ever expanding caseloads toward identifying genuine need and directing resources where they have the greatest chance of improving lives.
If the goal is better outcomes rather than larger bureaucracies, the focus must return to careful diagnosis, targeted treatment, and meaningful recovery wherever possible. Only by realigning incentives with those goals can the system ensure that children and families facing severe autism receive the attention and support they truly need.
My wife (retired from pediatric practice) used to have to battle school administrators, who *wanted* autism diagnoses to be made, when in her judgment the diagnosis did not pertain. She had happy parents in her office and angry school nurses on the phone in subsequent days. They were incentivized to increase the number of students with this diagnosis, as it meant more money for their school district. She occasionally encountered parents who welcomed the diagnosis, as it came with perks such as tutoring and extended time to take tests.
When I made this point as a response to a Facebook post (not one that you had made), a Facebook friend went nuclear on me, misinterpreting what I had said as an implicit indictment of her son’s autism diagnosis. I hope a similar fate does not await you.